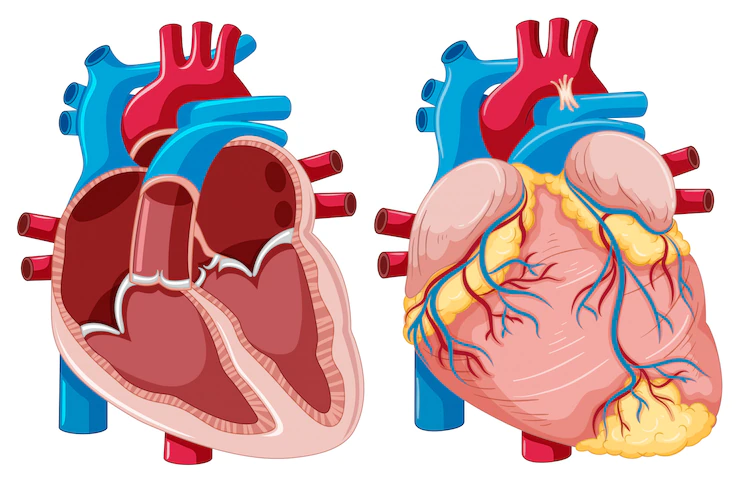
Coronary Artery Aneurysms – Overview Of Diagnosis And Management
Coronary artery aneurysms (CAAs) are rare and are defined as a localized dilatation of a coronary artery segment that is more than 1.5 times larger than neighboring normal segments.
Author:Suleman ShahReviewer:Han JuJul 24, 2022149 Shares2K Views

Coronary artery aneurysms(CAAs) are rare and are defined as localized dilatation of a coronary artery segment that is more than 1.5 times larger than neighboring regular segments.
Coronary artery aneurysms have a prevalence ranging from 0.3 to 5.3%. Coronary artery aneurysms have been increasingly identified in coronary angiography since the advent of the interventional era.
Risk factors are atherosclerosis, Takayasu arteritis, congenital diseases, Kawasaki disease (KD), and percutaneous coronary intervention.
Coronary artery aneurysms' natural historyis unknown; nevertheless, some recent research has proposed the underlying molecular pathways, and genome-wide association studies have identified various genetic predispositions to coronary artery aneurysms.
There is still debate over how to treat coronary artery aneurysms, and new research supports the necessity of early detection in patients susceptible to coronary artery aneurysms, such as children with Kawasaki disease.
What Are Coronary Artery Aneurysms?
Coronary artery aneurysms are 1.5-fold larger dilatations in the coronary artery than regular neighboring segments. Coronary artery ectasias, on the other hand, manifest as widespread arterial dilatations in which the length of the dilated segment exceeds 50% of the diameter.
Aneurysms are classed as genuine or false based on the integrity of the vessel wall (pseudoaneurysms).
Pseudoaneurysms are dilatations of the vessel caused by rupture of the media and external elastic membrane, with single or double layers of the vessel wall. They are frequently caused by a direct blow to the chest or coronary intervention.
On the other hand, an arterial aneurysm is a fusiform or saccular dilation of the artery that involves all three layers of the vessel's tunica. Certain writers refer to dilations larger than 4 cm in diameter as enormous coronary aneurysms.
Causes Of Coronary Artery Aneurysms
Coronary Artery Disease
Atherosclerosis is the most prevalent cause of coronary artery aneurysms, accounting for 50% of those identified in adulthood.
According to the Coronary Artery Surgery Study (CASS) registry, individuals with aneurysms with associated coronary artery disease had a 4.9% prevalence, compared to 0.37-2.53% for patients with coronary artery stenoses.
Histopathological study of atherosclerotic coronary artery aneurysms showed hyalinization and lipid deposition, causing disruption of the arterial wall's intimal and medial layers and eliminating the elastic muscle components.
Long-term inflammation, localized regions of calcification and fibrosis, and massive cholesterol crystals weakened the artery walls even further.
Genetic Reasons
In individuals with coronary artery disease (CAD), the likelihood of developing coronary artery aneurysms has been connected to genetic variations on chromosome 9p21.3.
This locus has been linked to an altered proliferative phenotype that favors adverse vascular remodeling.
Given the comparative pathophysiology of coronary artery aneurysms and more prominent vessel disorders, further research is needed to determine the possible overlap in genetic predispositions to coronary artery aneurysms and atherosclerotic diseases.
Coronary artery aneurysm patients have a poorer prognosis than the general population, and risk stratification tools may offer crucial clinical information.
Percutaneous Coronary Interventions
Since the beginning of the interventional era, there has been rising worry regarding the incidence of coronary artery aneurysms after percutaneous coronary interventions for atherosclerotic coronary artery disease, including balloon angioplasty, stent implantation, and, in particular, the use of drug-eluting stents (DESs).
Stent Implantation
Thirty-four coronary artery aneurysms (0.76% per lesion) were found in 29 individuals during follow-up 414 213 days after drug-eluting stent implantation. Several methods have been suggested to explain how stent-related coronary artery aneurysms arise.
Using large, high-pressure balloons during percutaneous coronary interventions may result in vascular dissection. A drug-eluting stent has been demonstrated to enhance the risk of coronary artery aneurysms by delayed neointimal repair and reendothelization processes.
Drug-eluting stents are pre-treated with cytotoxic anti-restenosis medicines that inhibit smooth muscle and endothelial cell growth. Coronary artery aneurysms were discovered in 15 individuals after drug-eluting stent implantation.
The clinical manifestations of coronary artery aneurysms ranged from an abrupt myocardial infarction (in two individuals) to nine patients staying clinically quiet. The 1-year event-free survival rate was 49%, which was linked to the size of the coronary artery aneurysm.
Vasculitis
The most prevalent cause of coronary artery ectasias is Kawasaki illness (CAEs). Coronary artery aneurysms develop in around 10-15% of Kawasaki disease patients during the acute period.
TNF-alpha, an inflammatory cytokine, has been related to the etiology of coronary artery aneurysms in Kawasaki disease patients. GWAS may assist in identifying Kawasaki disease patients at a higher risk of developing coronary artery aneurysms and determining the amount of their vasculitis.
So far, genetic variants have been found that enhance the incidence of coronary artery aneurysms in Kawasaki disease patients by a minor amount. Transcription regulates Matrix Metalloproteinase expression through the prostaglandin E2-cAMP pathway.
Inflammatory cytokines may activate this pathway, causing an imbalance in Matrix Metalloproteinase levels. This imbalance is hypothesized to cause vessel wall matrix deterioration and coronary artery aneurysms.
Connective Tissue Disorders
Coronary artery aneurysms may also be caused by hereditary connective tissue illnesses such as Marfan syndrome and Ehlers-Danlos syndrome.
TGF-b receptor mutations have been linked to a higher risk of arterial aneurysms.
Neurofibromatosis is a congenital genetic disorder characterized by extensive neuroectodermal and mesodermal dysplasia affecting the neurological, skeletal, and vascular systems.
Infections And Drugs Use
Coronary artery aneurysm etiologies include bacterial, mycobacterial, fungal, syphilitic, Lyme, septic emboli, mycotic aneurysm, and HIV infections.
Coronary artery aneurysms in mycotic lesions are also caused by pathogen penetration into the vessel wall or immune complex deposition.
Several researchers have documented Mycotic coronary artery aneurysms following drug-eluting stent implantation. Coronary artery aneurysms are also caused by medications such as cocaine, protease inhibitors, and amphetamines.
Coronary artery aneurysm production in cocaine users may be triggered by severe hypertension episodes and direct endothelial damage caused by vasoconstriction.
Other Causes
Congenital coronary artery aneurysm is another cause of coronary artery aneurysms, accounting for 20-30% of all coronary aneurysms; however, the genesis of congenital coronary artery aneurysms is yet unknown.
Fibromuscular dysplasia (FMD), a non-atherosclerotic and non-inflammatory vascular disease frequently linked with lesions of the internal carotid and renal arteries, has also been identified in the coronary arteries.
A coronary artery aneurysm was documented as a complication of FMD of the intimal, medial, adventitial, and periarterial layers for the first time.
This event might help researchers better grasp the underlying mechanics of congenital coronary artery aneurysms.
How Are Coronary Artery Aneurysms Diagnosed?
Most individuals with coronary artery aneurysms are asymptomatic, and coronary artery aneurysms are often discovered accidentally during diagnostic coronary angiography.
Non-invasive methods like echocardiography, CT, and MR imaging may also identify coronary artery aneurysms.
The ideal exam would assess the distribution, maximum diameter, and presence or absence of intraluminal thrombi.
Coronary Angiography
Coronary angiography gives vital information on aneurysm size, shape, location, frequency, and degree of coronary artery atherosclerosis.
Coronary angiography may identify thrombotic occlusions, evaluate the amount of collateral artery development, and examine any coronary artery stenoses.
Before recommending a patient for invasive angiography, it is critical to assess the procedure's advantages and hazards, especially in younger patients with Kawasaki disease.
While coronary angiography may not give further information in individuals with mild ectasia or tiny fusiform aneurysms, it may be helpful in patients with more complicated coronary diseases.
Furthermore, traditional angiography is confined to a "luminogram." It does not reflect information about the arterial wall, which might lead to an overestimate of aneurysm size or possibly miss a coronary artery aneurysm that is obstructed by a big thrombus or plaque.
The capacity of coronary angiography to distinguish between a true aneurysm and a pseudoaneurysm is likewise restricted.
Intravascular Ultrasound
Intravascular ultrasonographymay be used in the invasive angiographic examination of coronary artery aneurysms, and coronary artery aneurysm therapycan begin simultaneously.
The "gold standard" for giving important anatomical information to solve the diagnostic constraints of assessing coronary aneurysms during angiography has become intravascular ultrasound.
Intravascular ultrasonography produces transmural pictures of the coronary arteries, enabling the extraction of information on the arterial wall anatomy and luminal composition. This is critical for distinguishing the many kinds of aneurysms, each of which has a different prognosis.
Intravascular ultrasound may also determine the link between a coronary aneurysm and a previously implanted stent. This is crucial considering the recent correlation of coronary artery aneurysms with percutaneous coronary procedures.
When a stent is inserted to repair a coronary dissection, aneurysms may form outside the stent struts. Intravascular ultrasound may also identify structural or functional changes in the coronary artery wall during cardiac catheterization.
When examined with intravascular ultrasound, the angiographically observed regressed coronary artery aneurysms show the exceptional intima-media complex thickness and a diminished vasoactive response to vasodilators.
The long-term clinical ramifications of these morphological and functional alterations are unclear, but they may highlight critical aspects in the natural history of coronary artery aneurysms.
Intravascular ultrasound may also be utilized during coronary artery aneurysm therapy, an essential tool in directing aneurysm coverage.
CT Angiography
The multidetector-row computed tomography (MDCT) technologyhas recently sparked renewed interest in non-invasive coronary angiography.
CT data may be rebuilt to offer information on the nature of the dilatation in the coronary channel, such as maximal diameter, shape, morphology, existence of any concomitant stenosis, plaque composition, and location concerning the surrounding vasculature.
The limitations of coronary angiography in identifying coronary aneurysms (i.e., underestimating coronary artery aneurysm size in the presence of intraluminal thrombi) have prompted researchers to consider CTCA's potential significance in diagnosing coronary artery aneurysms.
CTCA offers a quick three-dimensional examination that aids in comprehending complicated anatomic features, such as those observed in ectasia associated with coronary fistulas.
While coronary angiography can diagnose and treat coronary artery aneurysms, CTCA might be utilized to monitor individuals with suspected or treated coronary artery aneurysms. This approach requires radiation exposure and the use of iodinated contrast material.
Echocardiography
Transthoracic echocardiography and transesophageal echocardiography are two further non-invasive approaches for diagnosing coronary artery aneurysms.
Echocardiography is a promising imaging technique for assessing the cardiac aftermath of Kawasaki disease in children because of its non-invasive nature and high sensitivity and specificity for identifying anomalies in the proximal LMCA and RCA.
Echocardiography provides for a quantitative evaluation of internal vessel diameters, revealing the location of aneurysms and the presence or absence of intraluminal thrombi.
The type of the aneurysm may be determined by the relationship between the axial and lateral diameters of the coronary arteries.
Along with coronary angiography, echocardiography is a practical, non-invasive approach for guiding the long-term follow-up of these individuals into adulthood; it has also been claimed that the choice to do angiography may be driven by echocardiographic imaging of coronary arteries.
Coronary MR Angiography
As children get older, echocardiographic examination becomes more restricted; coronary magnetic resonance angiography is a viable option.
Magnetic resonance angiography can define coronary artery aneurysms in proximal coronary artery segments, providing flow rate and type inputdiagnosing.
More research is required to determine the reliability of magnetic resonance angiography in diagnosing coronary artery aneurysms and stenoses in distal arterial segments.
Treatment Of Coronary Artery Aneurysms
There is no agreement on the best way to manage coronary artery aneurysms, and the treatment options for coronary artery aneurysms include surgical, percutaneous, and medicinal treatments.
Treatment options should be individualized to each patient, considering various factors such as clinical presentation, etiology, aneurysm size, location, and period of expansion.
Medical Treatment
Early detection and treatment of Kawasaki disease-associated coronary artery aneurysms have been linked to a greater rate of coronary artery aneurysm regression and a reduced risk of significant adverse cardiovascular events.
Patients with atherosclerosis should undergo medical treatment based on guidelines to reduce their coronary artery disease risk factors.
The probable relationship between inflammatory cytokines, Matrix Metalloproteinase, and coronary artery aneurysms may suggest a function for statins and renin-angiotensin system inhibition.
If thrombosis and embolism are a concern, antiplatelet and anticoagulant medication should be explored long-term.
Percutaneous Intervention
In certain circumstances, a choice to omit the aneurysm might be taken to avoid future difficulties.
When making a choice, it is critical to consider both the immediate and long-term dangers associated with percutaneous procedures or surgery and the issues that may develop with long-term antithrombotic medication, such as bleeding.
When percutaneous exclusion is chosen, covered stents are indicated for people with the appropriate anatomy.
However, issues about using covered stents should still be addressed, such as lower deliverability, the risk of restenosis and thrombosis, and blockage of side branches.
Coil insertion is another percutaneous treatment option for wide-necked aneurysms.
Coil herniation, on the other hand, might cause blockage of the parent artery; hence, stent-assisted procedures are favored.
Another danger is aneurysm rupture during manipulation of the microcatheter, coils, or wires.
Surgery
For individuals who cannot be treated percutaneously, surgery is an option. It is also recommended for patients with obstructive coronary artery disease or those with large saccular aneurysms at a high risk of rupturing.
Several techniques may be used during surgery, including aneurysm resection, proximal and/or distal ligation, aneurysmal thrombectomy, and aneurysmectomy with or without bypass grafting.
People Also Ask
What Is Z Score In Kawasaki Disease?
Dilated coronary arteries have a Z score between +2.0 and +2.5 (i.e., 2 to 2.5 standard deviations above the average standardized for body surface area).
A minor aneurysm is a coronary artery with a Z score between +2.5 and less than +5.0.
Is An Aneurysm Coronary Heart Disease?
A coronary artery aneurysm is an abnormal dilation of a portion of the coronary artery. This uncommon condition affects between 0.3-4.9 percent of people who undergo coronary angiography.
How Is A Coronary Artery Aneurysm Treated?
Medical care, surgical excision, coronary bypass grafting (CABG), and percutaneous coronary procedures are all treatment possibilities (PCI).
However, the doctor faces a clinical quandary while managing these patients owing to a lack of randomized studies or societal guidelines.
What Causes Coronary Artery Aneurysm?
Atherosclerosis, Takayasu arteritis, congenital abnormalities, Kawasaki disease (KD), and percutaneous coronary intervention are all potential causes.
Conclusion
Coronary artery aneurysms are uncommon, yet they may be deadly in patients. Coronary artery aneurysms are typically related to coronary artery disease, and there is rising worry about coronary artery aneurysm formation after percutaneous coronary procedures.
The diagnosis of coronary artery aneurysms is predicted to rise as the use of angiography, high-resolution CT, and MRI becomes more ubiquitous; hence, solid evidence-based therapeutic techniques are essential.

Suleman Shah
Author
Suleman Shah is a researcher and freelance writer. As a researcher, he has worked with MNS University of Agriculture, Multan (Pakistan) and Texas A & M University (USA). He regularly writes science articles and blogs for science news website immersse.com and open access publishers OA Publishing London and Scientific Times. He loves to keep himself updated on scientific developments and convert these developments into everyday language to update the readers about the developments in the scientific era. His primary research focus is Plant sciences, and he contributed to this field by publishing his research in scientific journals and presenting his work at many Conferences.
Shah graduated from the University of Agriculture Faisalabad (Pakistan) and started his professional carrier with Jaffer Agro Services and later with the Agriculture Department of the Government of Pakistan. His research interest compelled and attracted him to proceed with his carrier in Plant sciences research. So, he started his Ph.D. in Soil Science at MNS University of Agriculture Multan (Pakistan). Later, he started working as a visiting scholar with Texas A&M University (USA).
Shah’s experience with big Open Excess publishers like Springers, Frontiers, MDPI, etc., testified to his belief in Open Access as a barrier-removing mechanism between researchers and the readers of their research. Shah believes that Open Access is revolutionizing the publication process and benefitting research in all fields.

Han Ju
Reviewer
Hello! I'm Han Ju, the heart behind World Wide Journals. My life is a unique tapestry woven from the threads of news, spirituality, and science, enriched by melodies from my guitar. Raised amidst tales of the ancient and the arcane, I developed a keen eye for the stories that truly matter. Through my work, I seek to bridge the seen with the unseen, marrying the rigor of science with the depth of spirituality.
Each article at World Wide Journals is a piece of this ongoing quest, blending analysis with personal reflection. Whether exploring quantum frontiers or strumming chords under the stars, my aim is to inspire and provoke thought, inviting you into a world where every discovery is a note in the grand symphony of existence.
Welcome aboard this journey of insight and exploration, where curiosity leads and music guides.
Latest Articles
Popular Articles