Q Waves On ECG – A New Diagnostic Tool In Cardiology
Q waves on ECG are the deflection of the QRS complex that is initially negative. A Q wave technically signifies that the net direction of early ventricular depolarization (QRS) electrical forces projects toward the negative pole of the lead axis under consideration.
Author:Suleman ShahReviewer:Han JuAug 09, 202248 Shares648 Views
A Q wavetechnically signifies that the net direction of early ventricular depolarization(QRS) electrical forces projects toward the negative pole of the lead axis under consideration.
Although strong Q waves are a hallmark of myocardial infarction, they may also be seen in various non-infarct conditions.
Failure to recognize the different origins of Q waves might result in significant diagnostic mistakes.
A Q wave does not suggest any particular electrophysiological process.
Q waves, on the other hand, may be linked to one or more of the elements: (i) Effects of physiology and place, (ii) Myocardial damage or replacement, and (iii) Ventricular hypertrophy.
What Is Q Wave?
The QRS complex begins with the Q wave, the first downward deflection following the P wave.
There is no Q wave when the initial deflection of the QRS complex is vertical.
In many, but not all, ECG leads, a typical person will have a modest Q wave.
More than 75% of normal people have small Q waves in their left precordial leads. They are most common in lead V6, less often in leads V5 and V4, and seldom in V3. Q waves in these leads are more common in younger participants than in older people.
When the transitional zone lies on the right side of the precordium, Q waves are more likely to be present.
The Q waves last no more than 0.03 seconds. The amplitude is typically less than 0.2 mV, although it may reach 0.3 mV or even 0.4 mV.
Young adults get deeper Q waves more often. Teenagers may experience amplitudes of 0.4 mV or more.
Q wave length of ≥0.03 second was seen in 20% of normal male individuals in the posterior leads V7-V9.
Q wave abnormalities are usually suggestive of myocardial infarction and are explored further in the appropriate parts of ECG.
The names "Q wave myocardial infarction" and "non-Q wave myocardial infarction" was formerly used to describe various kinds of MIs that resulted in either Q wave development or the lack of Q wave development.
Pathological Q Waves
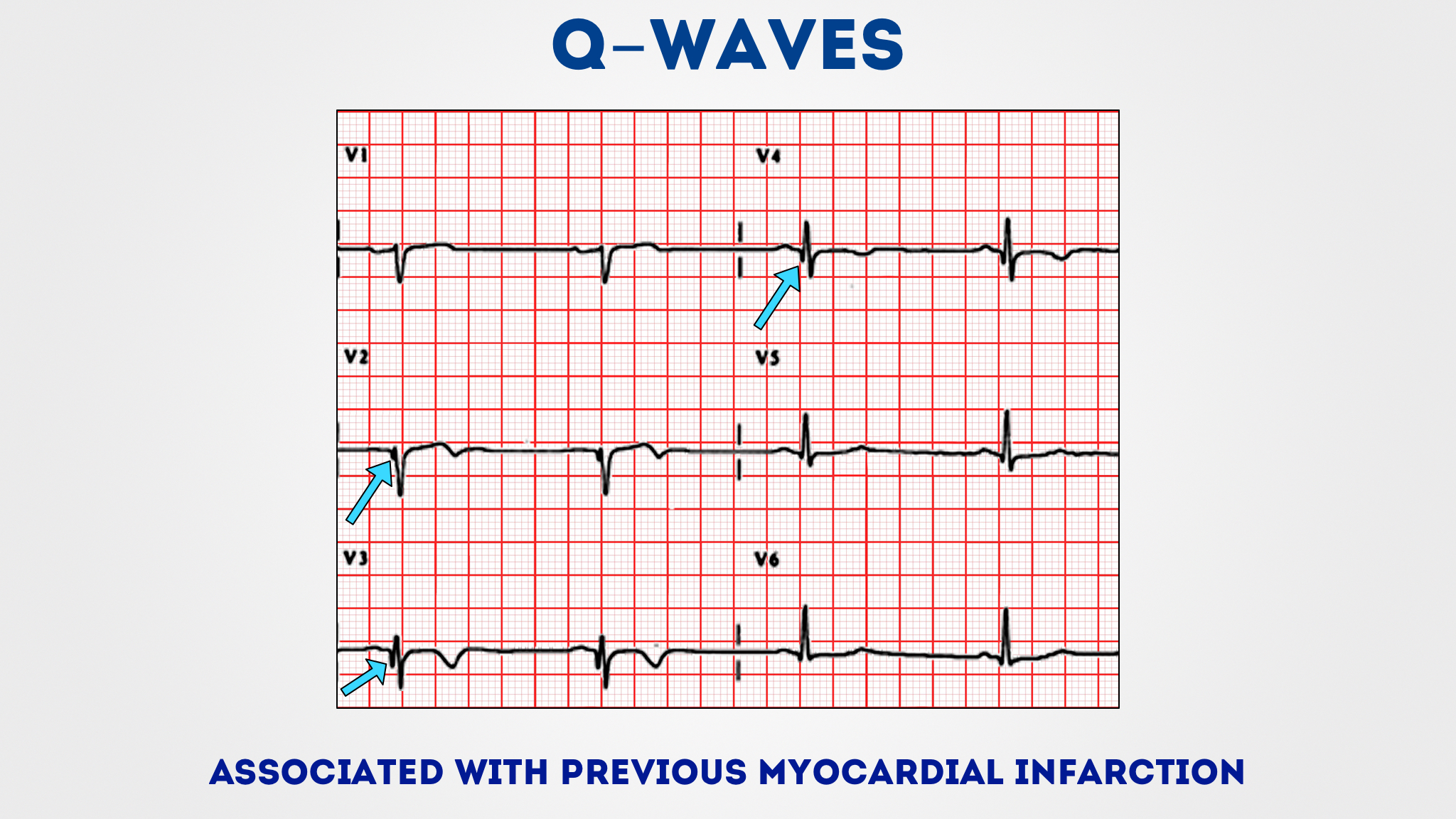
Pathologic Q waves indicate a prior myocardial infarction.
A lack of electrical activity causes them. A myocardial infarction may be seen as an electrical 'hole' since scar tissue is electrically dead, resulting in pathologic Q waves.
Pathologic Q waves are not an early indicator of myocardial infarction; they often develop over many hours to days.
Once pathogenic Q waves have formed, they seldom disappear.
If the myocardial infarction is reperfused early (for example, as a consequence of percutaneous coronary intervention), shocked myocardial tissue may recover, and pathologic Q waves dissipate.
In all other cases, they usually last eternally.
The exact definition of pathologic Q waves has been questioned.
Q waves are deemed abnormal if and only if the following conditions are met:
- > 40 ms (1 mm) broad
- > 2 mm deep
- > 40 ms (1 mm) broad
- seen in leads V1-3
Pathological Q waves generally imply a recent or previous myocardial infarction.
Q Waves And Myocardial Infarctions
Normal conduction occurs when ventricular depolarization goes from left to right through the septum and subsequently across both ventricles, with net forces directed towards the bigger left ventricle.
Posterior myocardial infarctions does not create Q-waves on the 12 lead (unless it is accompanied with inferior or lateral myocardial infarctions), but rather towering R waves in the anterior leads. Right sided leads contain small positive R waves and bigger negative S waves in a normal ECG, but left sided leads might have tiny negative "septal Q" waves.
New Q-waves may appear as soon as one hour following the onset of ischemic symptoms and are related with bigger infarcts, decreased EF, and increased mortality.
A study of STEMI patients treated within six hours of symptom onset found that 39% remitted.
According to the 2017 ESC recommendation, "the existence of Q-wave on the ECG does not necessarily affect the reperfusion approach."
Q Wave In The Inferior Leads
Q waves may be seen on the 12-lead ECG on a regular basis owing to heart axis disease such as subacute myocardial infarction, myocardial scar, or accessory pathways.
Other entities, such as restricted hypertrophy, may sometimes cause strong Q waves and serve as an essential differential diagnosis, particularly in younger individuals.
In the case of unusual chest discomfort, determining the precise diagnosis might be difficult.
To minimize unneeded intrusive operations, localized hypertrophy should be considered.
The Q wave on the surface ECG reflects a septum excitation from left to right.
Small Q waves may develop depending on the cardiac axis, for example, in leads I and aVL with a left axis or in leads II, III, and aVF with an inferior or right axis.
A pathological Q wave may be caused by a local deviation in electrical excitation caused by cardiac scarring.
The presence of Q waves in the inferior leads often indicates a subacute inferior myocardial infarction, an inferior wall scar, or the existence of an inferior auxiliary route.
Due to anatomic axis deviation, a more pronounced Q wave has also been documented during the second and third trimesters of normal pregnancy.
The limited hypertrophy of the basal anterior wall is the fundamental source of the strong Q wave.
In a small group of 17 pediatric patients, a hypertrophic nonobstructive cardiomyopathy was previously recognized as a probable cause of Q wave.
An aberrant Q wave in the inferior leads was seen in 75% of individuals with ventricular anterior septum hypertrophy.
This points to limited hypertrophy as a crucial differential diagnosis for substantial inferior Q waves, particularly in younger people.

Abnormal Q Waves In Adults
Abnormal Q waves on an ECG are often attributed to an underlying myocardial infarction.
The effectiveness of abnormal Q waves in diagnosing myocardial infarction as an inadequately specific indicator of myocardial infarction is dependent on its prevalence in the population examined.
In one research, 82 people under the age of 40 with abnormal Q waves were compared to 82 participants beyond the age of 40 with comparable abnormal Q waves to identify the presence or absence of cardiac disease or myocardial infarction.
Cardiac disease was present in 90.2% of the younger and 92.7% of the older patients, respectively, but myocardial infarction was present in only 15.9% of the younger and 68.3% of the older subjects.
The causes of heart illness vary between younger and older people. Some forms of abnormal Q waves were more beneficial than othersin determining whether myocardial infarction was present or not.
Abnormal Q waves were a robust predictor of organic heart disease in both adult age groups, although their value in predicting myocardial infarction varied with age.
Myocardial infarction was found in a tiny percentage of patients under 40 years old with abnormal Q waves in the group investigated, but was more common in older subjects with identical abnormal Q waves.
Is Abnormal Q Wave Dangerous?
Q waves that appear in the subacute phase of myocardial infarction and continue into the chronic phase frequently indicate myocardial necrosis.
However, the mechanism and relevance of Q waves that arise relatively early in the course of acute myocardial infarction (within 6 hours of beginning of symptoms), particularly when accompanied with ST elevation, are likely to be different.
In patients with anterior myocardial infarction, abnormal Q waves on the admission ECG are related with greater peak creatine kinase, a higher frequency of heart failure, and an increased mortality.
Patients with inferior myocardial infarction who have abnormal Q waves on their admission ECG do not have a poor prognosis.
Q Waves And Heart Attack
Q-waves on the ECG are a substantial predictor of mortality or hospitalization for ischaemic heart disease in the general population without established cardiac disease, independent of age, hypertension, diabetes, or renal function.
Even modest Q waves had a poor prognosis; there was no difference in result between anterior and posterior position.
Large Q-waves were characterized using the Minnesota Code Classification System, which was first used in Circulation in 1960.
To the best of our knowledge, this is the first research to show that the amount of the necrotic region of infarction influences prognosis even in the situation of undiagnosed myocardial infarction.
The influence of front vs. posterior position of identified myocardial infarctions on prognosis has been widely researched.
This is the first research to compare the differences between anterior and posterior undetected myocardial infarctions.
The location of Q-waves had no effect on prognosis, indicating that undiagnosed posterior infarctions are just as dangerous as anterior ones.
The ECG has more leads (I, aVL, V1-V6) covering the front wall than the posterior wall (II, III, aVF).
This might be due to the fact that each anterior lead represents a smaller portion of the left ventricle.
Although smoking, plasma cholesterol levels, and body mass index (BMI) are all established risk factors for ischaemic heart disease, there is no link between them and undiagnosed myocardial infarction.
Other disorders, such as pre-excitation of the ventricles, might cause abnormal Q-waves on the ECG.
Unrecognized myocardial infarction is highly related with age, diabetes, hypertension, and compromised renal function.
This shows that these disorders may obscure the usual signs of myocardial infarction, increasing the likelihood of it going undiagnosed.

People Also Ask
What Does Q Wave In Lead 3 Mean?
Q waves in leads III and aVF cannot be classified as positional or aberrant based on their alterations during deep inspiration.
Q waves in the inferior leads indicate a myocardial infarction of the lower, or usually posterior, and occasionally laterally positioned, left ventricular wall.
What Do Abnormal Q Waves Indicate?
The early phase of ventricular depolarization is represented by Q waves.
If they are extremely broad (>0.2 second) or abnormally deep (>5 mm), they are pathogenic. Pathologically deep but not broad Q waves are often indicative of ventricular hypertrophy.
What Causes Abnormal Q Waves On ECG?
Abnormal Q waves on an ECG are often associated with an underlying myocardial infarction.
What Happens During Q Wave?
The electrical stimulus begins to depolarize the septum from left to right as it goes through the His bundle and before it divides down the two bundle branches.
When Do Q Waves Appear?
Q waves may arise one to two hours after the commencement of symptoms of an acute myocardial infarction, although they usually require 12 hours and can present up to 24 hours later.
The existence of pathogenic Q waves, on the other hand, does not always imply a total infarct.
Conclusion
Even small and especially large Q waves on ECGof individuals who do not have known ischaemic heart disease or heart failure are associated with a significant risk of ischaemic heart disease and death.
Any such Q-wave may indicate the need for further investigation in order to detect asymptomatic cardiovascular diseaseand institute proper medical and potentially invasive or surgical treatment.

Suleman Shah
Author
Suleman Shah is a researcher and freelance writer. As a researcher, he has worked with MNS University of Agriculture, Multan (Pakistan) and Texas A & M University (USA). He regularly writes science articles and blogs for science news website immersse.com and open access publishers OA Publishing London and Scientific Times. He loves to keep himself updated on scientific developments and convert these developments into everyday language to update the readers about the developments in the scientific era. His primary research focus is Plant sciences, and he contributed to this field by publishing his research in scientific journals and presenting his work at many Conferences.
Shah graduated from the University of Agriculture Faisalabad (Pakistan) and started his professional carrier with Jaffer Agro Services and later with the Agriculture Department of the Government of Pakistan. His research interest compelled and attracted him to proceed with his carrier in Plant sciences research. So, he started his Ph.D. in Soil Science at MNS University of Agriculture Multan (Pakistan). Later, he started working as a visiting scholar with Texas A&M University (USA).
Shah’s experience with big Open Excess publishers like Springers, Frontiers, MDPI, etc., testified to his belief in Open Access as a barrier-removing mechanism between researchers and the readers of their research. Shah believes that Open Access is revolutionizing the publication process and benefitting research in all fields.

Han Ju
Reviewer
Hello! I'm Han Ju, the heart behind World Wide Journals. My life is a unique tapestry woven from the threads of news, spirituality, and science, enriched by melodies from my guitar. Raised amidst tales of the ancient and the arcane, I developed a keen eye for the stories that truly matter. Through my work, I seek to bridge the seen with the unseen, marrying the rigor of science with the depth of spirituality.
Each article at World Wide Journals is a piece of this ongoing quest, blending analysis with personal reflection. Whether exploring quantum frontiers or strumming chords under the stars, my aim is to inspire and provoke thought, inviting you into a world where every discovery is a note in the grand symphony of existence.
Welcome aboard this journey of insight and exploration, where curiosity leads and music guides.
Latest Articles
Popular Articles