Septum Cavum Pellucidum – Prevalence And Risks In Childern
Septum cavum pellucidum is a possible space between the septum pellucidum's membrane leaves separated by at least 1 mm and is considered a typical anatomical variation.
Author:Suleman ShahReviewer:Han JuJul 09, 2022116 Shares2.1K Views
Septum cavum pellucidumis a possible space between the septum pellucidum's membrane leaves separated by at least 1 mm and is considered a typical anatomical variation.
It contains a cerebrospinal fluid filtrate transported from the ventricles through the septal laminae and has no communication with the subarachnoid space.
It may sometimes connect to a more posterior cavity termed cavum vergae, although they are separated by an arbitrary vertical plane produced by the fornix columns.
In the past, septum cavum pellucidum and cavum vergae were wrongly referred to as the fifth and sixth ventricles. Both are not part of the ventricular system since they have a separate embryological origin and lack an ependymal or choroid plexus lining.
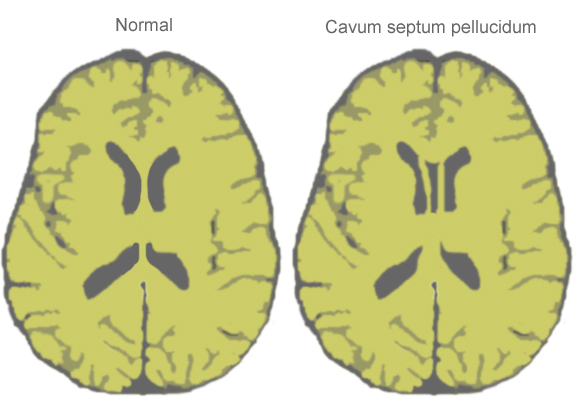
The septum pellucidum is a thin, triangular, double membrane that separates the frontal horns of the right and left ventricles. Its apex is near the foramen of Monro, and its base is towards the quadrigeminal cistern. A septum cavum pellucidum cyst is described as a fluid-containing entity between lateral ventricles at least 10 mm wide or has ventricular wall lateral bending.
Septum Cavum Pellucidum Function
The septum pellucidum (Latin for "translucent wall"), also known as the ventricle of Sylvius, is a thin, triangular double membrane that separates the frontal horns of the brain's right and left lateral ventricles. Its breadth ranges from 1.5 to 3.0 mm and spans between the anterior section of the corpus callosum and the body of the fornix.
The septum pellucidum is a vital limbic system component connecting to the medial and basolateral limbic circuits. Diseases affecting the septum cavum pellucidum might induce symptoms via a mass impact or disrupt the limbic system's emotional and behavioral activities.
Is Cavum Septum Pellucidum Dangerous?
Despite popular belief, the septum pellucidum is more than merely a neuronal tract that links the corpus callosum and fornix. As shown by symptoms of mental retardation and learning difficulties found with septum pellucidum lesions, it is a comlimbic system component that works as a relay station to the primary hippocampus and hypothalamus nuclei.
Superiorly, the inferior surface of the corpus callosum's body; anteroinferiorly, the superior surface of the corpus callosum's genu; posteroinferiorly, the corpus and columns of the fornix; laterally, the medial wall of the frontal horns of the lateral ventricles; and medially, the virtual space between the contralateral septum.
The cavum septum pellucidumis a common anatomic variation that is frequently asymptomatic and only identified by chance. Cavum vergae is the name given to the CSP's posterior expansion.
The septum cavum pellucidum prevalence rapidly drops after birth, reaching 85% at one month, 45% at two months, and 15% at three to six months. It closes caudally to rostrally, resulting in the obliteration of the caudal part first (at 38 weeks of gestation).
The anterior section only disappears by three to six months of age, owing to the fast expansion of the corpus callosum and hippocampus alvei, as well as the concrescence of cerebral hemispheres, which leads to the fusion of the septum pellucidum membranes. Cavum vergae is found in around 30% of neonates and remains in just 1% of adults.
The septum cavum pellucidum cysts are characterized as communicative or non-communicating based on their communication with the ventricles. Secondary communications may develop due to head trauma, surgery, or spontaneous rupture. Cavum septum pellucidum cysts may potentially be asymptomatic (incidental) or symptomatic.
The most prevalent and persistent symptom associated with septum cavum pellucidum cysts is headache, which is caused by intermittent hydrocephalus caused by postural changes and other movements that increase intracranial pressure (Valsalva, straining, etc.).
Septum cavum pellucidum cysts are an uncommon but critically significant source of possibly reversible positional headaches. Asymmetric lateral ventricle cysts with bowed but intact septum pellucidum, a vein of Galen aneurysm, cavum septum arachnoid cyst, and an interhemispheric cyst related to agenesis of corpus callosum and cavum velum interpositum are among the differential diagnoses for anterior intracranial midline cysts.
Septum Cavum Pellucidum Symptoms
The benign midline anterior intracranial cysts, septum cavum pellucidum cyst, cavum vergae, and cavum velum interpositum have different appearances.
They are pathological when they cause symptoms, which vary depending on the size of the cysts. Septum cavum pellucidum cysts are very uncommon, occurring just 0.04% of the time. Septum cavum pellucidum symptomatic cysts are much more unusual, with just a few occurrences recorded in the literature.
A septum cavum pellucidum cyst may cause headaches, focal neurological impairments, ataxia, seizures, papilledema, emesis, syncope, visual, and even sensorimotor abnormalities.
Gradually growing cysts may cause visual, behavioral, or autonomic problems. While most septum cavum pellucidum cysts are found by chance, they tend to stay asymptomatic despite the bulk impact. The most prevalent symptom, however, is headache, and a direct relationship to the cyst becomes an exclusion diagnosis.
Septum Cavum Pellucidum Diagnosis
The septum pellucidum (SP) is produced in the folds of the primordium hippocampus during the eighth week of embryonic development and is crossed by the corpus callosum (CC). The laminae are two membranes that make up the lateral ventricle's wall. It is a component of the limbic system that is filled with cerebrospinal fluid.
According to numerous studies, the absence of septum pellucidum is an uncommon brain illness with a frequency in the general population ranging between 2 and 3/100,000 people. The lack of septum pellucidum is caused by the SP's septal disruption or agenesis. It might also be partial or total, congenital or acquired.
The absence of septum pellucidum (ASP) is an uncommon condition that affects brain anatomy. It is either solitary or linked to a variety of congenital brain abnormalities. A second-trimester ultrasound may be used to diagnose ASP.
Prenatal counseling is hopeful about neurological prognosis when the ASP is isolated, although there is a 20% chance of septooptic dysplasia in the neonate.

Septum pellucidum tumor differential diagnosis
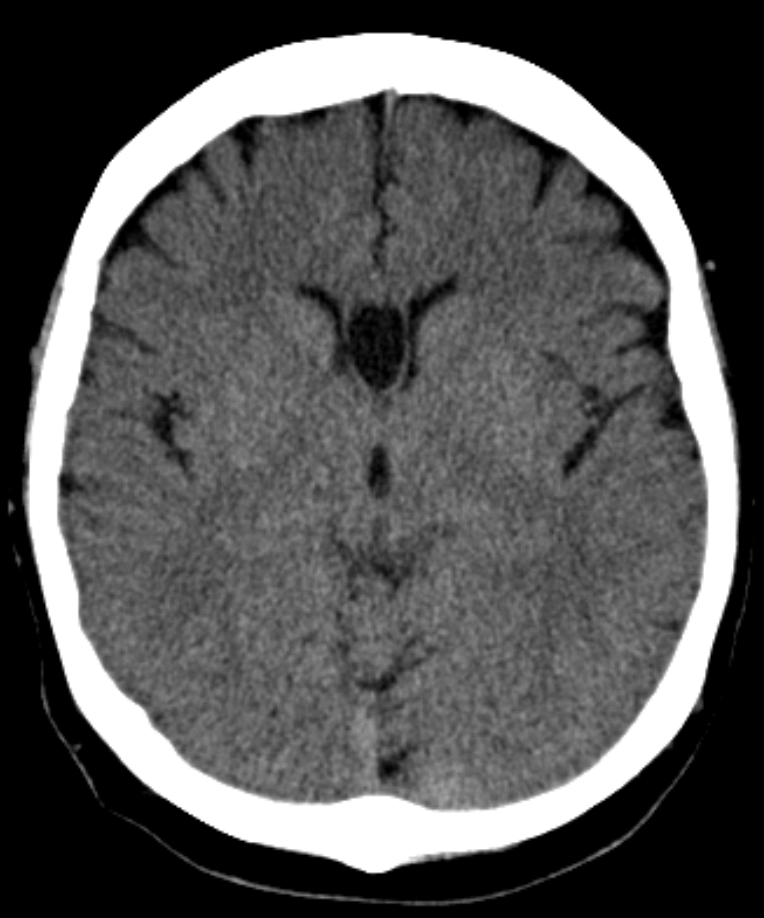
Cavum Septum Pellucidum Radiology
The imaging of a normal cavum septi pellucidi (CSP) is a significant marker in the fetal brain's second and third-trimester prenatal ultrasonographyexamination, providing confidence in normal central forebrain development.
Non-visualization of the CSPseptum cavum pellucidum is a prenatal sonographic abnormality usually linked with neuroanatomical defects such as corpus callosum agenesis, schizencephaly, septo-optic dysplasia, holoprosencephaly, chronic hydrocephalus, and acquired fetal brain damage.
The isolated septal deficit, an uncommon but contentious condition, is seen as a variety of ordinary. Columns of the fornix that imitate septum cavum pellucidum and conspicuous cavum vergae that might simulate non-visualization of the septum cavum pellucidum are typical difficulties in the sonographic assessment of septum cavum pellucidum.
When the septum cavum pellucidum is not visible, the fetal brain's magnetic resonance imaging (MRI) may confirm and assess related abnormalities.
Septum Cavum Pellucidum Treatment
The following conditions are treated for cavum septum pellucidum:
- The presence of a septum cavum pellucidum cyst on imaging examinations and clinical signs and symptoms due to a blockage of cerebrospinal fluid passage in the foramen of Monro.
- The cyst's direct compression of surrounding tissues
- Changes in mental state or localized neurological impairments caused by the septum cavum pellucidum cyst.
In open surgical procedures, conventional shunting and stereotactic fenestration are the standard treatments in these situations.
Dandy documented the first treated septum cavum pellucidum cyst in 1931, when he performed a transcallosal fenestration on a 4.5-year-old kid.
Since the initial endoscopic technique was published in 1995, neuroendoscopic fenestration has become a well-established therapeutic alternative and is now the therapy of choice for symptomatic septum cavum pellucidum cysts.
There are three endoscopic methods described:
- 1.A frontal approach on the coronal suture 3 cm from the midline, targeting the lateral ventricle's frontal horn (used by the majority of authors)
- 2.The same cortical frontal technique is used, but this time the cyst is directly targeted, and the two walls are fenestrated.
- 3.An occipital burr hole to optimize the trajectory into the atrium of the lateral ventricle, allowing a perpendicular access to both leaflets of the cyst.
Endoscopic fenestration is a less intrusive procedure that provides direct vision and efficacy. Inadvertent harm is avoided via direct viewing of neuronal and circulatory systems.
It is also critical to examine the Monro foramina for any adhesions that may be causing the hydrocephalus to remain after the cyst has been successfully drained. Furthermore, this approach eliminates the requirement for a shunt and allows for a biopsy of the cyst walls.
The presence of septum cavum pellucidum and cavum vergae may influence cerebral endoscopic surgical route selection, with the transcavum interforniceal path favored over the transforaminal approach into the third ventricle.
Symptomatic cavum septum pellucidum hypertrophy is uncommon and most usually produces intermittent obstructive hydrocephalus with headache and loss of consciousness. It may be treated surgically by cyst puncture or shunting, ventriculoperitoneal shunting, or radical excision.
Cavum septum pellucidum is a vital sign for assessing proper fetal neural axis development.
People Also Ask
Does Everyone Have Cavum Septum Pellucidum?
A cavum septum pellucidum is present in a normal fetus, but over 85% of them fuse by 3-6 months of age, implying that a cavum septum pellucidum remains in 15% of adults.
At What Age Does The Cavum Septum Pellucidum Close?
The cavum is present in all newborns. However, it usually closes within 5 months.
How Do You Treat Cavum Septum Pellucidum?
Many cavum septum pellucidum cysts are surgically treated; conservative therapy is seldom advised.
What Does The Cavum Septum Pellucidum Do?
Diseases affecting the cavum septum pellucidum might induce symptoms via a mass impact or disrupt the limbic system's emotional and behavioral activities.
Conclusion
Although uncommon, a cyst of cavum septum pellucidum may be considered in the differential diagnosis when a patient exhibits symptoms associated with a blockage of cerebrospinal fluid flow. After endoscopic fenestration of the cyst, the symptoms are entirely resolved, confirming the link between headache and cavum septum pellucidum cyst.

Suleman Shah
Author
Suleman Shah is a researcher and freelance writer. As a researcher, he has worked with MNS University of Agriculture, Multan (Pakistan) and Texas A & M University (USA). He regularly writes science articles and blogs for science news website immersse.com and open access publishers OA Publishing London and Scientific Times. He loves to keep himself updated on scientific developments and convert these developments into everyday language to update the readers about the developments in the scientific era. His primary research focus is Plant sciences, and he contributed to this field by publishing his research in scientific journals and presenting his work at many Conferences.
Shah graduated from the University of Agriculture Faisalabad (Pakistan) and started his professional carrier with Jaffer Agro Services and later with the Agriculture Department of the Government of Pakistan. His research interest compelled and attracted him to proceed with his carrier in Plant sciences research. So, he started his Ph.D. in Soil Science at MNS University of Agriculture Multan (Pakistan). Later, he started working as a visiting scholar with Texas A&M University (USA).
Shah’s experience with big Open Excess publishers like Springers, Frontiers, MDPI, etc., testified to his belief in Open Access as a barrier-removing mechanism between researchers and the readers of their research. Shah believes that Open Access is revolutionizing the publication process and benefitting research in all fields.

Han Ju
Reviewer
Hello! I'm Han Ju, the heart behind World Wide Journals. My life is a unique tapestry woven from the threads of news, spirituality, and science, enriched by melodies from my guitar. Raised amidst tales of the ancient and the arcane, I developed a keen eye for the stories that truly matter. Through my work, I seek to bridge the seen with the unseen, marrying the rigor of science with the depth of spirituality.
Each article at World Wide Journals is a piece of this ongoing quest, blending analysis with personal reflection. Whether exploring quantum frontiers or strumming chords under the stars, my aim is to inspire and provoke thought, inviting you into a world where every discovery is a note in the grand symphony of existence.
Welcome aboard this journey of insight and exploration, where curiosity leads and music guides.
Latest Articles
Popular Articles