Umbilical Hernia – How It Affects Women During Pregnancy
The umbilical hernia occurs when a section of the abdominal lining, part of the intestine, and/or fluid from the abdomen pass through the abdominal wall muscle.
Author:Suleman ShahReviewer:Han JuJul 03, 202212 Shares319 Views

Women are more likely than males to have an umbilical hernia. Because of the steadily increased intra-abdominal pressure, pregnancy may induce herniation or make an existing one visible. An umbilical hernia occurs in 0.08% of pregnant women. Umbilical hernia repair during pregnancy may be done with little risk to the mother and the baby.
The second trimester is an ideal time for surgery. Asymptomatic umbilical hernia may be treated after delivery or a cesarean section (C-section). Elective repair after delivery is achievable as early as the eighth week postpartum. A one-year interval may provide the patient with a fairly smooth recovery, including hormonal stability and resumption of average body weight.
Furthermore, if the patients want additional children, surgery may be postponed for a longer period, even after another pregnancy. Diastasis recti are relatively common during pregnancy. It may last throughout the postpartum phase. Patients with rectus diastasis are at significant risk of recurrence. This risk is particularly important after suture repairs. In this case, mesh repairs should be considered.
What Is Umbilical Hernia?
An umbilical hernia is an abnormal protrusion at the umbilicus that may be seen or felt (belly button). The umbilical hernia occurs when a section of the abdominal lining, part of the intestine, and/or fluid from the abdomen pass through the abdominal wall muscle.
Umbilical hernias are most frequent in babies, although they may also occur in adults. An umbilical hernia in a newborn is more noticeable when the child screams, causing the belly button to protrude. This is a common symptom of an umbilical hernia.
Umbilical hernia in children often closes on their own during the first two years of life, while some may stay open until the fifth year or beyond. Adult-onset umbilical hernias are more likely to need surgical correction.
Umbilical hernia causes a soft swelling or bulging at the navel, the bulge in a baby with an umbilical hernia may be seen only when they scream, cough, or stretch.
Children's umbilical hernias are generally painless. Umbilical hernias that develop in maturity may cause stomach pain.
What Causes Umbilical Hernia In Adults
The umbilical cord passes through a hole in the baby's belly during pregnancy (tummy). This gap should resolve quickly after delivery; however, the muscles may not entirely shut in rare situations.
This causes a weakness in the muscle wall around it (abdominal wall). An umbilical hernia occurs when fatty tissue or a portion of the colon protrudes into the region surrounding the navel.
Factors that might lead to the development of an umbilical hernia in adults include:
- being fat or overweight
- squeezing when lifting or carrying large goods
- having a chronic heavy cough
- having twins or triplets as a result of multiple pregnancies
Umbilical Hernia Treatment In Adults
Surgery is the only technique to heal a hernia in adults. Without treatment, umbilical hernias may become more painful and larger.
For people with symptomatic hernias, most clinicians advocate surgery. Adults with umbilical hernias are often repaired with hernia mesh by surgeons. There are two forms of surgery for hernia repair: open hernia repair and laparoscopic hernia repair.
- In open hernia repair, surgeons make an incision at the spot and use mesh or sutures to reinforce the abdominal wall or closure the hernia. The muscle layer will subsequently be sutured closed.
- To do laparoscopic hernia repair, physicians create tiny incisions and introduce instruments through the small holes. Surgeons may treat the hernia using mesh or stitches. This procedure is more challenging and costly, but it may result in a faster recovery for patients.
Umbilical Hernia During Pregnancy
Women are more likely than males to have umbilical hernias. Because of the steadily growing intra-abdominal pressure, pregnancy may produce an umbilical hernia or make an existing one visible. Most individuals have hernia symptoms throughout the second trimester. A hernia might be discovered during the first, second, or third pregnancy. In a recent large series, the incidence of an umbilical hernia in pregnant women was as low as 0.08 percent. However, complex instances such as a full-term pregnancy in umbilical hernia, peritonitis owing to skin ulceration, or an imprisoned pregnant uterus inside the hernia rims might occur.
Yet, there is no clear surgical protocol for a pregnant lady with a hernia, although more and better scientific evidence has been accumulated. There is no agreement on the best time to have surgery for an umbilical hernia in a pregnant woman or expecting to become pregnant. In reality, these two sorts of situations should be treated individually. Hernias that are symptomless or have limited symptoms, such as slight discomfort or pain, should be evaluated regularly and treated electively after birth and uterine involution, according to Augustin and Majerovic. It has recently been shown that watching and waiting, even for up to 5 years, seems safe for ventral hernias in the adult population.

Postpartum Hernia, Causes, Signs and Symptoms, Diagnosis and Treatment.
Repairing Umbilical Hernia During C-Section
A popular surgical method is hernia repair during a C-section. However, until the 2000s, these combined procedures were not widely recorded. The first case series of C-sections with simultaneous inguinal or umbilical hernia surgeries was published in 2004. With their informed agreement, three patients were offered and received combination surgery. The existence of the umbilical hernia itself was an indicator for C-section in one of them. The length of operation was higher in instances with inguinal hernia repair but not in cases with umbilical hernia repair as compared to a C-section alone. Simultaneous umbilical hernia repair and cesarean took longer than just a cesarean.
Even in emergency situations, umbilical hernia surgerymay be accomplished with minimum morbidity to the mother and no fetal loss. Surgery should be performed during the second trimester if a minor hernia develops, and symptomatic umbilical hernias may be treated after delivery or a C-section. Patient satisfaction with combination C-section and hernia repair is great. However, a significant risk of recurrence is predicted.

Umbilical Hernia After Childbirth
Some pregnant women with umbilical hernias do not have hernia repair done simultaneously with the C-section. The cause for this might be a patient or surgeon's preference. Other risks regarding simultaneous surgery include the potential of local and systemic complications. During pregnancy, the rectus abdominis muscle's general anatomy changes.
The abdominal muscles' functional capacity is also changed, as is their ability to maintain the pelvis. It may be preferable to wait for the muscles to return to normal before fixing an umbilical hernia. Relaxin is an insulin-like peptide hormone released by the corpus luteum. It softens and expands the cervix while relaxing pelvic ligaments. Relaxin may contribute to the etiology of perineal hernia in dogs by promoting muscle atrophy and connective tissue degeneration.
After childbirth, elective repair is well documented. It can possible as early as 8 weeks postpartum. Small asymptomatic hernias in the early postpartum period do not need surgery. A one-year interval may provide the patient with a fairly smooth recovery, including hormonal stability and resumption of normal body weight. If the patient wishes to have additional children, surgery may be postponed for longer after another pregnancy.
Only one study found a link between relaxin and abdominal hernias in people. All infants born in Malmö, Sweden, were examined for congenital hip dislocation and an inguinal hernia for five years. There is no agreement on weight lifting restrictions after hernia procedures. However, surgeons advise their patients not to lift any weight for the first two weeks. In reality, carrying and raising a newborn would be within the guidelines. Small asymptomatic hernias do not need surgery in the early postpartum period. A one-year interval may provide the patient with a reasonably smooth recovery, including hormonal stability and resumption of average body weight.
Diastasis Recti
Diastasis recti are the separation of the rectus abdominal muscles in the midline. It is an impediment, but it is not an open hernia, and there is no chance of imprisonment. There is a relationship between parity and diastasis recti. During pregnancy, the prevalence is between 30 and 70%.
Diastasis recti are quite common during pregnancy. It may last throughout the postpartum period. After repair, patients with rectus diastasis may have umbilical hernia recurrence. This is particularly true after suture repairs. In this case, mesh repairs should be considered.
Although diastasis recti is not a hernia, it may reoccur as a bigger hernia after umbilical hernia procedures. Sutures pass the bites through a weak rectus sheet in the diastasis area. This may result in rips and buttonhole flaws, leading to recurrence. If there is a susceptible linea alba owing to diastasis recti, it is reasonable to expect a recurrence from the locations of mesh fixation. In the event of the full restoration of the line alba, it is preferable to utilize no fixation or an autraumatic mesh fixation such as glues (e.g., fibrin) or a self-gripping mesh in retro muscular mesh repairs.
People Also Ask
What Symptoms Can An Umbilical Hernia Cause?
- A bulge in or around the belly button becomes greater as you strain, raise, or cough.
- Pressure or discomfort at the location of the hernia.
- Constipation.
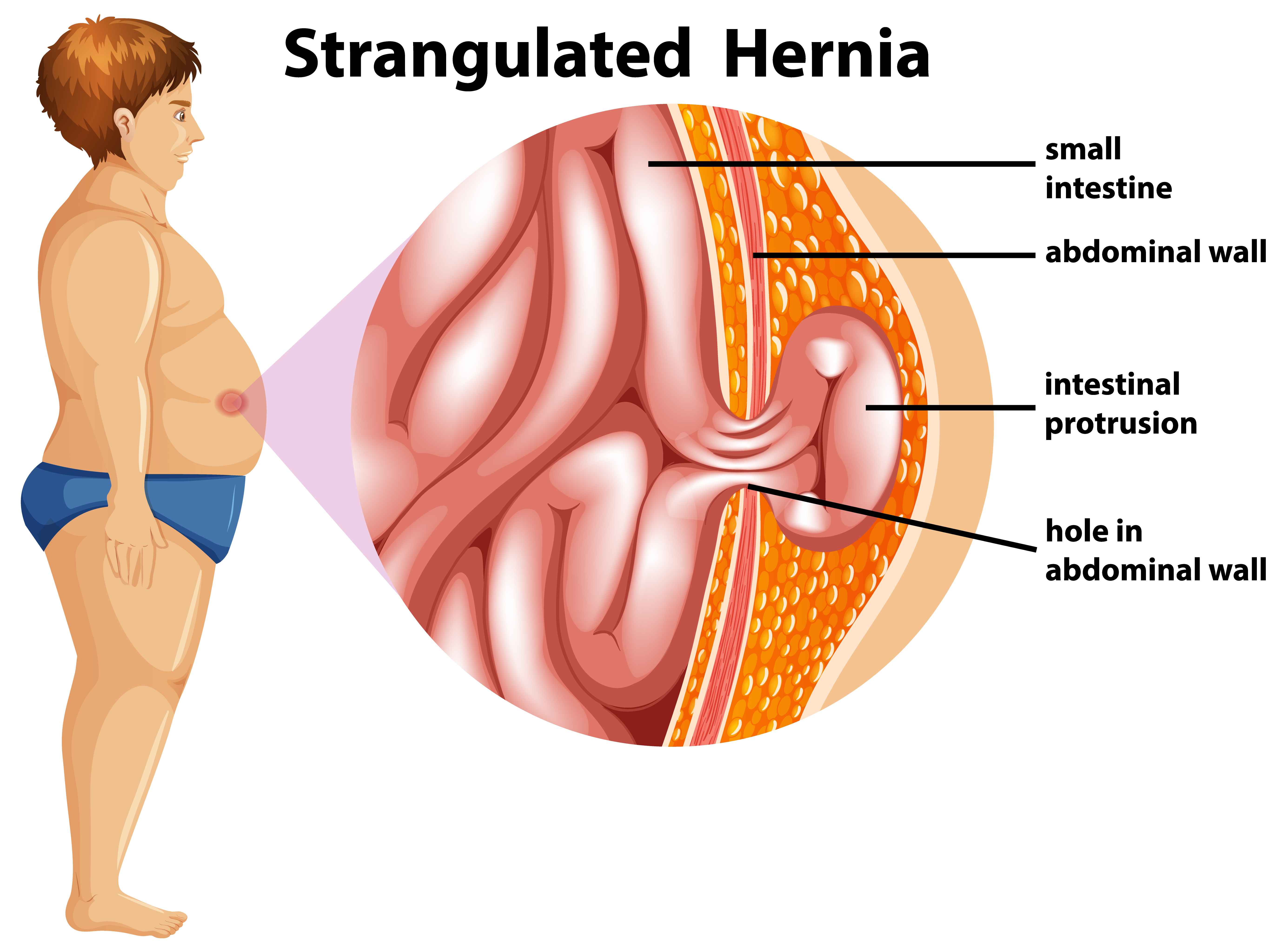
- Sharp stomach discomfort with vomiting might indicate a strangulated hernia, a medical emergency.
Can Umbilical Hernias Go Away?
No, an umbilical hernia will not disappear on its own. Only surgery can fix it.
How Do You Treat A Umbilical Hernia?
An umbilical hernia can only be repaired surgically. An umbilical hernia repair operation helps reposition the sac and reinforce the abdominal wall.
How Serious Is An Umbilical Hernia?
An umbilical hernia is not inherently hazardous, but it may get stuck (incarcerated). This may cut off the blood supply to the contents of the hernia, resulting in potentially fatal complications, including gangreneor peritonitis (if this happens, the hernia is said to be strangulated).
Conclusion
There is no agreement on the best time to have surgery for an umbilical hernia in a pregnant woman or expecting to become pregnant. An emergency repair is unavoidable if the hernia is incarcerated or strangulated at the time of diagnosis. An elective repair should be suggested if the hernia is not complex but causing symptoms. If the hernia is treated with sutures, the chance of recurrence during pregnancy is significant. Mesh repair may limit the flexibility of the abdominal wall and induce discomfort during a future pregnancy. When the patient has a small and asymptomatic hernia, it may be best to wait until she delivers birth before repairing it.

Suleman Shah
Author
Suleman Shah is a researcher and freelance writer. As a researcher, he has worked with MNS University of Agriculture, Multan (Pakistan) and Texas A & M University (USA). He regularly writes science articles and blogs for science news website immersse.com and open access publishers OA Publishing London and Scientific Times. He loves to keep himself updated on scientific developments and convert these developments into everyday language to update the readers about the developments in the scientific era. His primary research focus is Plant sciences, and he contributed to this field by publishing his research in scientific journals and presenting his work at many Conferences.
Shah graduated from the University of Agriculture Faisalabad (Pakistan) and started his professional carrier with Jaffer Agro Services and later with the Agriculture Department of the Government of Pakistan. His research interest compelled and attracted him to proceed with his carrier in Plant sciences research. So, he started his Ph.D. in Soil Science at MNS University of Agriculture Multan (Pakistan). Later, he started working as a visiting scholar with Texas A&M University (USA).
Shah’s experience with big Open Excess publishers like Springers, Frontiers, MDPI, etc., testified to his belief in Open Access as a barrier-removing mechanism between researchers and the readers of their research. Shah believes that Open Access is revolutionizing the publication process and benefitting research in all fields.

Han Ju
Reviewer
Hello! I'm Han Ju, the heart behind World Wide Journals. My life is a unique tapestry woven from the threads of news, spirituality, and science, enriched by melodies from my guitar. Raised amidst tales of the ancient and the arcane, I developed a keen eye for the stories that truly matter. Through my work, I seek to bridge the seen with the unseen, marrying the rigor of science with the depth of spirituality.
Each article at World Wide Journals is a piece of this ongoing quest, blending analysis with personal reflection. Whether exploring quantum frontiers or strumming chords under the stars, my aim is to inspire and provoke thought, inviting you into a world where every discovery is a note in the grand symphony of existence.
Welcome aboard this journey of insight and exploration, where curiosity leads and music guides.
Latest Articles
Popular Articles