Humeral Head – How To Treat Its Fractures
Because supraspinatus is attached to the humeral head, the insertional angle at which the tendon contacts the bone varies significantly when abduction occurs.
Author:Suleman ShahReviewer:Han JuJun 25, 202227 Shares421 Views
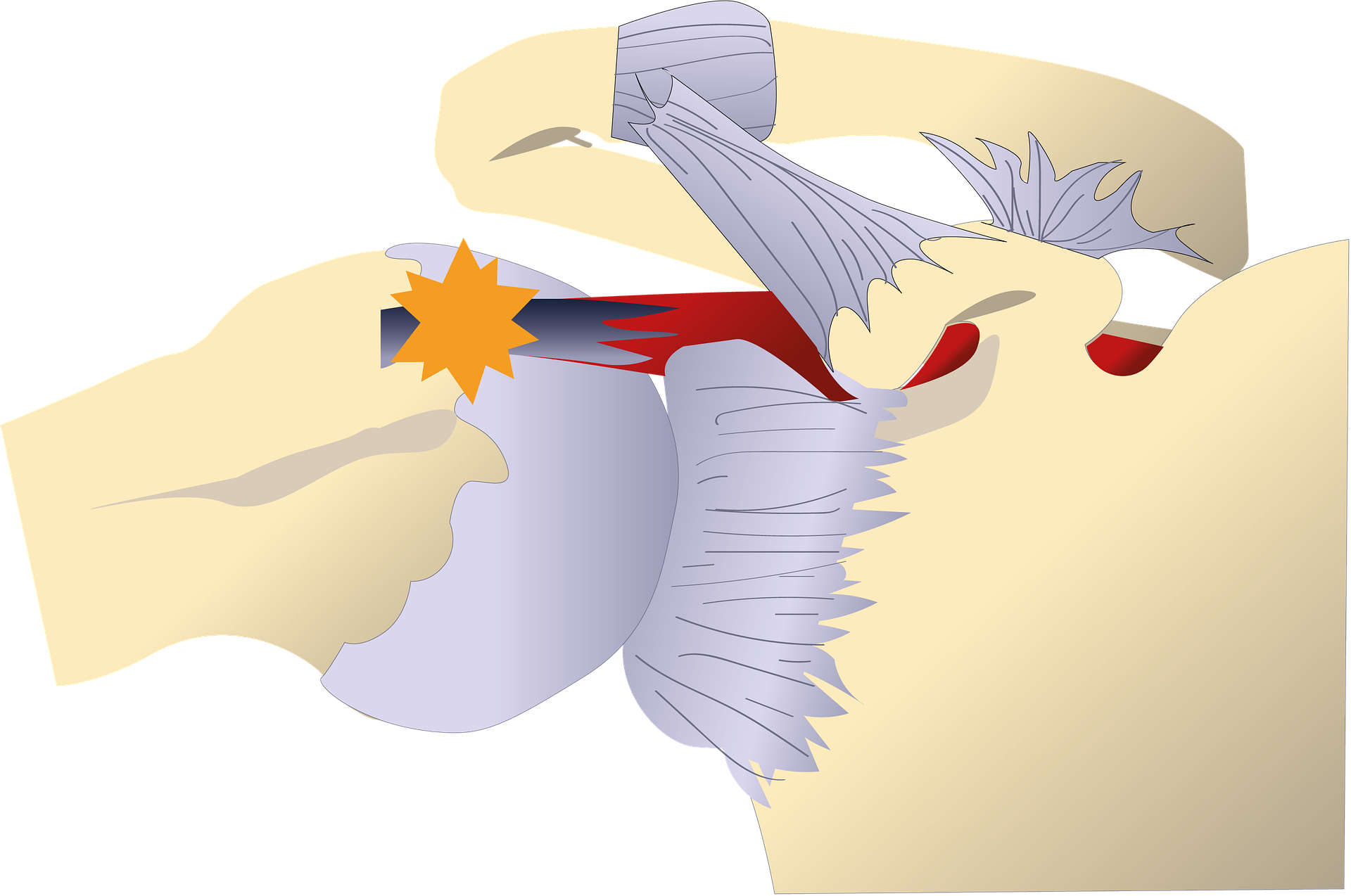
Because supraspinatus is attached to the humeral head, the insertional angle at which the tendon contacts the bone varies significantly when abduction occurs.
The shape of the humeral head (caput humeri) is roughly hemispherical. The glenohumeral joint is formed by articulating the scapula's glenoid cavity with the scapula's glenoid cavity (shoulder joint). The circumference of its articular surface is somewhat restricted and referred to as the anatomical neck, as opposed to the surgical neck, which is typically the fracture site. Anatomical neck fractures are uncommon. In general, males have a bigger humeral head diameter than women.
Humeral Head Osteonecrosis
Humeral head osteonecrosis is an uncommon but major cause of shoulder discomfort that often does not respond well to non-surgical treatment. The humeral head gets its blood supply through complicated anastomoses that branch from the axillary artery, which explains why it has a lower risk of osteonecrosis than other articulations like the hip. The anterior and posterior circumflex arteries, which branch from the axillary artery in various ways, are the principal providers of vascularity to the humeral head.
The anterior circumflex artery goes laterally under the long head of the biceps and branches as the arcuate artery, which reaches the proximal humerus near the upper end of the bicipital groove and supplies both the lesser and greater tuberosities. The posterior circumflex artery goes around the posterior humeral neck and culminates in tiny perforating branches. It is not as adherent to the humeral head as the anterior artery.
Humeral Head Fractures
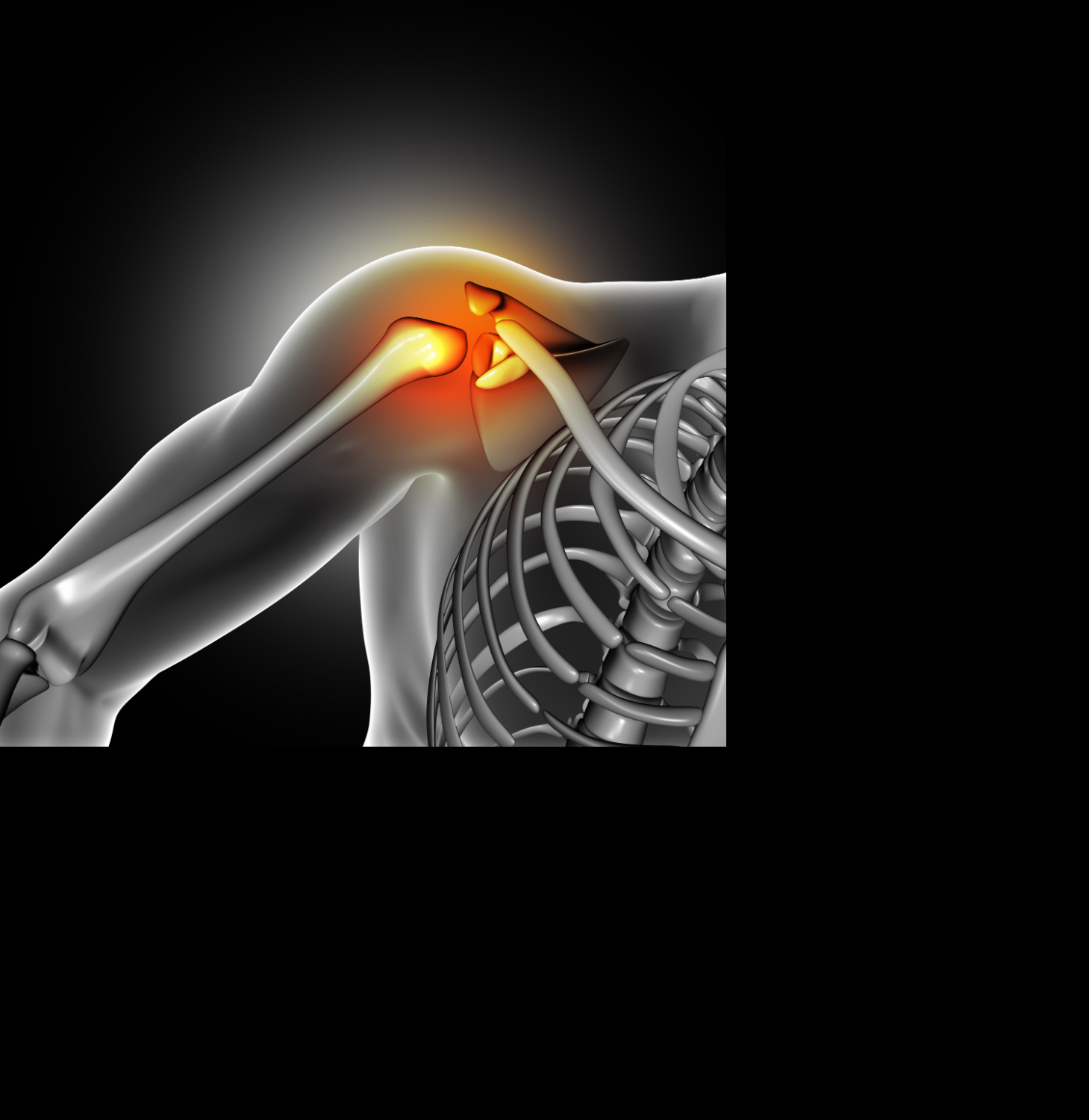
A proximal humeral fracture is a break in the region around the humeral head, also known as the ball of the ball-and-socket joint of the shoulder. The humeral head is placed near the humerus's tip (upper arm bone). A proximal humerus fracture may significantly impact the shoulder joint and upper arm mobility.
A shoulder fracture in the proximal head of the humerus may develop (upper arm bone). A proximal head fracture may develop as a ring around the anatomical neck or at one of the greater and lesser trochanters sites.
A proximal humeral fracture may produce upper arm discomfort, edema, and bruising down to the elbow. Other signs and symptoms may include:
- Shoulder mobility is restricted.
- The afflicted arm or hand is numb.
- Deformity of the upper arm.
Proximal humeral fractures are a common form of fracture that is most often found in the elderly. Experts estimate that 105 and 342 proximal humeral fractures occur per 100,000 persons annually.
Humeral Head Function
The humerus head is a component of the ball-and-socket shoulder joint. This location also acts as the insertion place for the shoulder girdle muscles. This contains the long head of the biceps tendon, as well as the rotator cuff muscles supraspinatus, infraspinatus, teres minor, and subscapularis.
The humerus collaborates with these muscles to raise and lower the upper arm (also known as flexion and extension), elevate laterally and lower (also known as abduction and adduction), move the arm in tiny and large circular movements (also known as circumduction), and spin inward or outward (also called internal rotation and external rotation).
Many ligaments are also present in this location to help secure the muscles as well as enable mobility to the shoulder joint.
The brachial plexus is a huge network of nerves that runs over the front section of the humerus.
This delivers feeling and motion to every muscle in the arm and parts of the neck and spinal cord.
Humeral Head Fracture Radiology
Plain films are generally enough for characterizing proximal humeral fractures and determining therapy. If good views cannot be acquired, if the fractures are uncommon, or if additional fractures (e.g., glenoid) are present, CT may be beneficial. Furthermore, CT (mainly 3D surface shaded reconstructions) has increased interobserver agreement on proximal humeral fracture classification.
Regardless of the imaging technique utilized, the number of displaced pieces should be counted to tooperly classify the fracture (Neer classification or AO classification are most commonly used).
Typically, the fracture is visible as a lucency and cortical breach with varying degrees of angulation, impaction, and displacement.
Humeral Head Fracture Treatment
Most proximal humerus fractures may be managed without surgery if the bone pieces are not displaced (displaced). Surgery is often undertaken to allow for early movement if the pieces become misaligned. Other considerations, however, are addressed while selecting between surgical fixing and nonoperative therapy.
Nonoperative therapy usually consists of a sling or shoulder immobilizer for the first two weeks, with no shoulder motion. Following that, the patient will be given weekly exercises to enhance the range of motion in the shoulder gradually ensure that the fracture is mending correctly; an X-ray of the shoulder will be done weekly or biweekly (every two weeks)
During surgery, the fractures are frequently fixed with plates, screws, or pinslder replacement may be required for severe fractures with recent arthroscopy (joint degeneration). Physical therapy is started shortly after surgery to help with mobility.
Depending on the fracture pattern and concomitant complications, a humerus shaft fracture may be treated surgically or nonsurgically (i.e., nerve injury or open fracture). For the first few days, a temporary splint reaching from the shoulder to the forearm and keeping the elbow bent at 90 degrees might be utilized to treat the fracture.
Nonoperative therapy often consists of fracture bracing that is replaced three to four weeks later by a cylinder brace (Sarmiento brace) that fits the upper arm while leaving the elbow free. The doctor will advise you on how long to wear the cast or splint and when to remove it. The fractured arm may take from weeks to months to recover entirely.
Rehabilitation is progressively increasing activity levels in order to reestablish muscular strength, joint mobility, and flexibility. Cooperation from the patient is critical to the rehabilitation process. On a daily basis, the patient must do range of motion, strengthening, and other activities specified by the doctor. Rehabilitation will continue until the muscles, ligaments, and other soft tissues are fully functional.
Internal fixation of the pieces using plates, screws, or a nail is often used in surgery. With no splints or casts, the rehabilitation varies little from nonoperative therapy. A sling is frequently supplied to the patient for comfort and arm support. Elbow activities may begin immediately after surgery. However, shoulder workouts may be postponed for a few weeks depending on the fracture pattern.
Risk For Humeral Head Fracture
Younger persons participating in high-impact sports or engaging in high-energy incidents may incur a humeral head fracture. These fractures may develop during contact sports such as football, gymnastics, and cycling, as well as car accidents and horseback riding falls. They are less common among players participating in non-contact sports such as baseball. Intense muscular spasms caused by a seizure or an electric shock are another cause of proximal humerus fractures and dislocations in children.
Humeral head fractures are most prevalent in elderly adults owing to decreased bone density (osteopeniaor osteoporosis) and may occur as a result of a low-impact fall, such as falling onto an extended hand. These are the third most prevalent form of fracture found in people over 65 and are more common in women.
People Also Ask
What Is Another Name For Humeral Head?
The humeral head is also known as caput humeri. The head (caput humeri) has a roughly hemispherical shape. The glenohumeral joint is formed by articulating the scapula's glenoid cavity with the scapula's glenoid cavity (shoulder joint).
What Causes Humeral Head Pain?
Traumatic disorders include shoulder fracture, dislocation, or surgery, which may result in humeral head necrosis. Atraumatic causes of humeral head osteonecrosis include corticosteroid usage, high alcohol use, sickle cell disease, divers' sickness, and other systemic disorders.
Where Is The Humeral Head?
The humerus bone is positioned between the shoulder and elbow joints in the upper arm. The glenohumeral joint, often known as the shoulder joint, is a ball and socket joint. The humeral head is represented by the ball, while the socket represents the glenoid fossa of the scapula.
What Is The Humeral Head?
The shoulder is a ball-and-socket joint, with the ball representing the rounded end of the humerus (humeral head) and the socket representing the cup section of the scapula (glenoid).
Conclusion
A thorough understanding of the path of the arteries feeding the humeral head may reduce the risk of vascular damage and eventual osteonecrosis. Because of the wide interindividual variability in vascular architecture, imaging studies before arthroscopic rotator cuff surgery may be recommended.
Therapy regimens supplied by an occupational or physical therapist will differ based on the documented impairments of each client. In overuse situations, these programs often involve splinting and exercise to enhance the upper arm and shoulder joint's coordination, strength, and range of motion.

Suleman Shah
Author
Suleman Shah is a researcher and freelance writer. As a researcher, he has worked with MNS University of Agriculture, Multan (Pakistan) and Texas A & M University (USA). He regularly writes science articles and blogs for science news website immersse.com and open access publishers OA Publishing London and Scientific Times. He loves to keep himself updated on scientific developments and convert these developments into everyday language to update the readers about the developments in the scientific era. His primary research focus is Plant sciences, and he contributed to this field by publishing his research in scientific journals and presenting his work at many Conferences.
Shah graduated from the University of Agriculture Faisalabad (Pakistan) and started his professional carrier with Jaffer Agro Services and later with the Agriculture Department of the Government of Pakistan. His research interest compelled and attracted him to proceed with his carrier in Plant sciences research. So, he started his Ph.D. in Soil Science at MNS University of Agriculture Multan (Pakistan). Later, he started working as a visiting scholar with Texas A&M University (USA).
Shah’s experience with big Open Excess publishers like Springers, Frontiers, MDPI, etc., testified to his belief in Open Access as a barrier-removing mechanism between researchers and the readers of their research. Shah believes that Open Access is revolutionizing the publication process and benefitting research in all fields.

Han Ju
Reviewer
Hello! I'm Han Ju, the heart behind World Wide Journals. My life is a unique tapestry woven from the threads of news, spirituality, and science, enriched by melodies from my guitar. Raised amidst tales of the ancient and the arcane, I developed a keen eye for the stories that truly matter. Through my work, I seek to bridge the seen with the unseen, marrying the rigor of science with the depth of spirituality.
Each article at World Wide Journals is a piece of this ongoing quest, blending analysis with personal reflection. Whether exploring quantum frontiers or strumming chords under the stars, my aim is to inspire and provoke thought, inviting you into a world where every discovery is a note in the grand symphony of existence.
Welcome aboard this journey of insight and exploration, where curiosity leads and music guides.
Latest Articles
Popular Articles